
Intro
Discover the 7 Siadh symptoms, including hyponatremia, headache, and nausea, and learn about Syndrome of Inappropriate Antidiuretic Hormone secretion causes, diagnosis, and treatment options for this rare hormonal disorder.
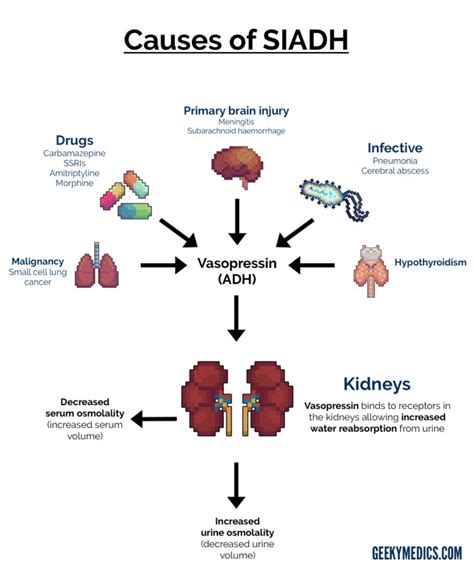
The syndrome of inappropriate antidiuretic hormone secretion, commonly referred to as SIADH, is a condition where the body produces an excessive amount of antidiuretic hormone (ADH), leading to water retention and resulting in a range of symptoms. Understanding these symptoms is crucial for early diagnosis and effective management of the condition. SIADH can arise from various causes, including certain medications, lung diseases, and neurological disorders, making its identification and treatment a complex process.
The importance of recognizing SIADH symptoms lies in their potential to mimic other conditions, sometimes leading to delayed or incorrect diagnoses. Furthermore, the inappropriate secretion of ADH can lead to significant imbalances in electrolytes, particularly hyponatremia (low sodium levels in the blood), which can be life-threatening if not addressed promptly. The management of SIADH involves correcting the underlying cause, managing fluid balance, and, in some cases, using medications to regulate ADH levels or improve the body's ability to excrete water.
Given the complexity and potential severity of SIADH, it is essential to delve into the specifics of its symptoms, causes, diagnosis, and treatment options. By understanding these aspects, healthcare providers and patients can work together to manage the condition effectively, preventing complications and improving outcomes. The following sections will explore the symptoms, diagnostic approaches, and treatment strategies for SIADH in detail, providing a comprehensive overview of this critical condition.
Introduction to SIADH Symptoms
SIADH symptoms can vary widely among individuals, depending on the severity of the condition and the underlying cause. Common symptoms include headache, nausea, vomiting, and fatigue, which can be attributed to the hyponatremia that often accompanies SIADH. In severe cases, patients may experience seizures or coma due to the critically low sodium levels. It is also important to note that some patients with SIADH may be asymptomatic, with the condition being discovered incidentally during routine blood tests.
Common Symptoms of SIADH
The clinical presentation of SIADH can be subtle, making it challenging for healthcare providers to diagnose the condition based solely on symptoms. However, several signs and symptoms are commonly associated with SIADH: - Headache: Due to water intoxication and hyponatremia. - Nausea and vomiting: Can be associated with the headache and overall feeling of being unwell. - Fatigue: A general feeling of tiredness that can be severe enough to interfere with daily activities. - Muscle weakness: Can be a consequence of severe hyponatremia. - Seizures: In severe cases, particularly if sodium levels drop very low. - Coma: A life-threatening complication of untreated, severe hyponatremia.Causes and Risk Factors of SIADH
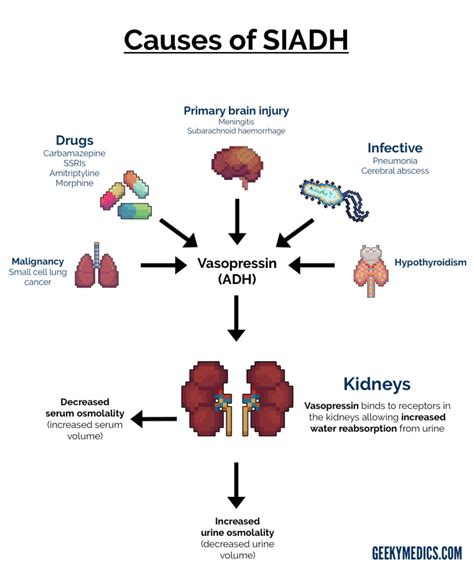
Understanding the causes and risk factors of SIADH is crucial for its prevention and management. The condition can be caused by a variety of factors, including:
- Medications: Certain drugs, such as selective serotonin reuptake inhibitors (SSRIs), carbamazepine, and vincristine, are known to induce SIADH.
- Lung diseases: Conditions like pneumonia, tuberculosis, and cystic fibrosis can lead to SIADH.
- Neurological disorders: Stroke, brain injury, and infections like meningitis can cause SIADH.
- Cancer: Tumors, especially small cell lung cancer, can produce ADH ectopically, leading to SIADH.
- Surgery: Postoperative SIADH can occur, particularly after thoracic or abdominal surgery.
Diagnosis of SIADH
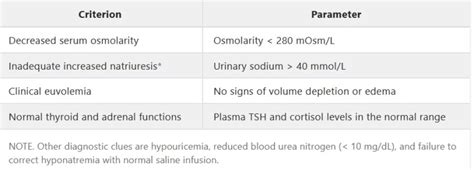
Diagnosing SIADH involves a combination of clinical evaluation, laboratory tests, and sometimes imaging studies. Key diagnostic criteria include: - Hyponatremia (usually <135 mmol/L) with euvolemia (normal blood volume). - Inappropriately elevated urine sodium concentration (>20-30 mmol/L). - Absence of clinical signs of volume depletion. - Normal or slightly elevated blood urea nitrogen (BUN) and creatinine levels. - Absence of other causes of hyponatremia, such as heart failure, liver disease, or renal disease.Treatment Options for SIADH
The treatment of SIADH focuses on correcting the water imbalance and addressing the underlying cause. Management strategies may include:
- Fluid restriction: The mainstay of treatment, aiming to reduce water intake to less than urine output.
- Medications: Vaptans (e.g., tolvaptan) can increase urine production and correct hyponatremia. Demeclocycline is an alternative that induces a state of nephrogenic diabetes insipidus, reducing the kidneys' response to ADH.
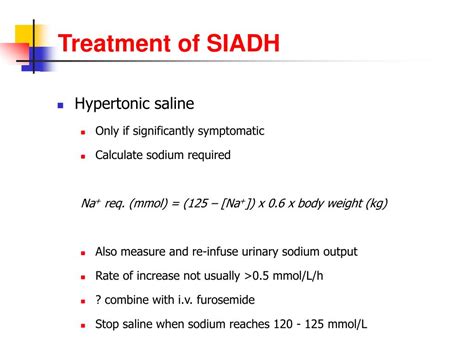
- Sodium supplements: In cases of severe hyponatremia, especially if symptomatic, intravenous sodium solutions may be used to correct sodium levels quickly.
- Addressing the underlying cause: Stopping offending medications, treating infections, or managing cancer can help resolve SIADH.
Complications of Untreated SIADH
Untreated SIADH can lead to severe complications, primarily due to hyponatremia. These include: - **Seizures:** Can occur if sodium levels drop too low. - **Coma:** A severe and potentially life-threatening complication. - **Brain damage:** Chronic or severe hyponatremia can lead to permanent neurological damage. - **Death:** In extreme cases, untreated SIADH can be fatal.Prevention and Management Strategies

Preventing SIADH involves avoiding or managing its risk factors. For individuals at risk, regular monitoring of sodium levels and clinical assessment for signs of SIADH can help in early detection. In cases where medications known to cause SIADH are necessary, close monitoring of electrolyte levels is recommended. Educating patients about the signs and symptoms of SIADH and the importance of adhering to treatment plans is crucial for effective management.
Future Directions in SIADH Management
Research into the pathophysiology of SIADH and the development of new therapeutic agents continues to evolve. Emerging treatments aim to more effectively manage hyponatremia and correct the underlying hormonal imbalances. Additionally, there is a growing interest in personalized medicine approaches, tailoring treatment to the individual's specific condition and response to therapy.Conclusion and Final Thoughts
In conclusion, SIADH is a complex condition that requires a comprehensive approach to diagnosis and management. Understanding its symptoms, causes, and treatment options is essential for healthcare providers and patients alike. By working together and staying informed about the latest developments in SIADH management, it is possible to improve outcomes and reduce the risk of complications. We invite readers to share their experiences, ask questions, and engage in discussions about SIADH, aiming to foster a community of support and knowledge sharing.
What are the primary symptoms of SIADH?
+The primary symptoms of SIADH include headache, nausea, vomiting, fatigue, and in severe cases, seizures or coma, primarily due to hyponatremia.
How is SIADH diagnosed?
+SIADH is diagnosed through a combination of clinical evaluation, laboratory tests (including serum and urine sodium levels), and sometimes imaging studies, with key criteria being hyponatremia, inappropriately elevated urine sodium, and absence of volume depletion.
What are the treatment options for SIADH?
+Treatment options for SIADH include fluid restriction, medications like vaptans or demeclocycline, and addressing the underlying cause. In severe cases, sodium supplements may be necessary to correct hyponatremia quickly.